Anxiety and Depression Disorders and Treatments
Note to students: The best preparation for taking the reading quiz is to pay close attention to the key terms as you read. Each question in the question banks is directly linked to these key terms and phrases.
Chapter Focus Question:
What is the nature and forms of anxiety disorder and what is the most effective therapies for curing them?
- Percentage of people with anxiety disorders
- Anxiety disorder
- Phobia
- Panic attacks
- Sources of panic attack
- Obsessive-compulsive disorder (OCD)
- Rituals for OCD
- Post-traumatic stress disorder (PTSD)
Section Focus Question:
What are anxiety disorders?
Key Terms:
Anxiety disorders are the most commonly diagnosed psychological disorders. By some estimates, the lifetime prevalence rate of these disorders is more than 20 percent in the United States. That means that in our lifetime 20 percent of us may be diagnosed with one of the problems we will describe below. Remember, this is more than you or I just feeling a little anxious from time to time. This is a level of problematic behavior that causes a significant amount of distress or causes impairment in our social role functioning, or both. This chapter will highlight some of the diagnosable anxiety disorders found in the DSM and the cognitive behavior therapy model used to understand and treat them.
Diagnosing Anxiety Disorders
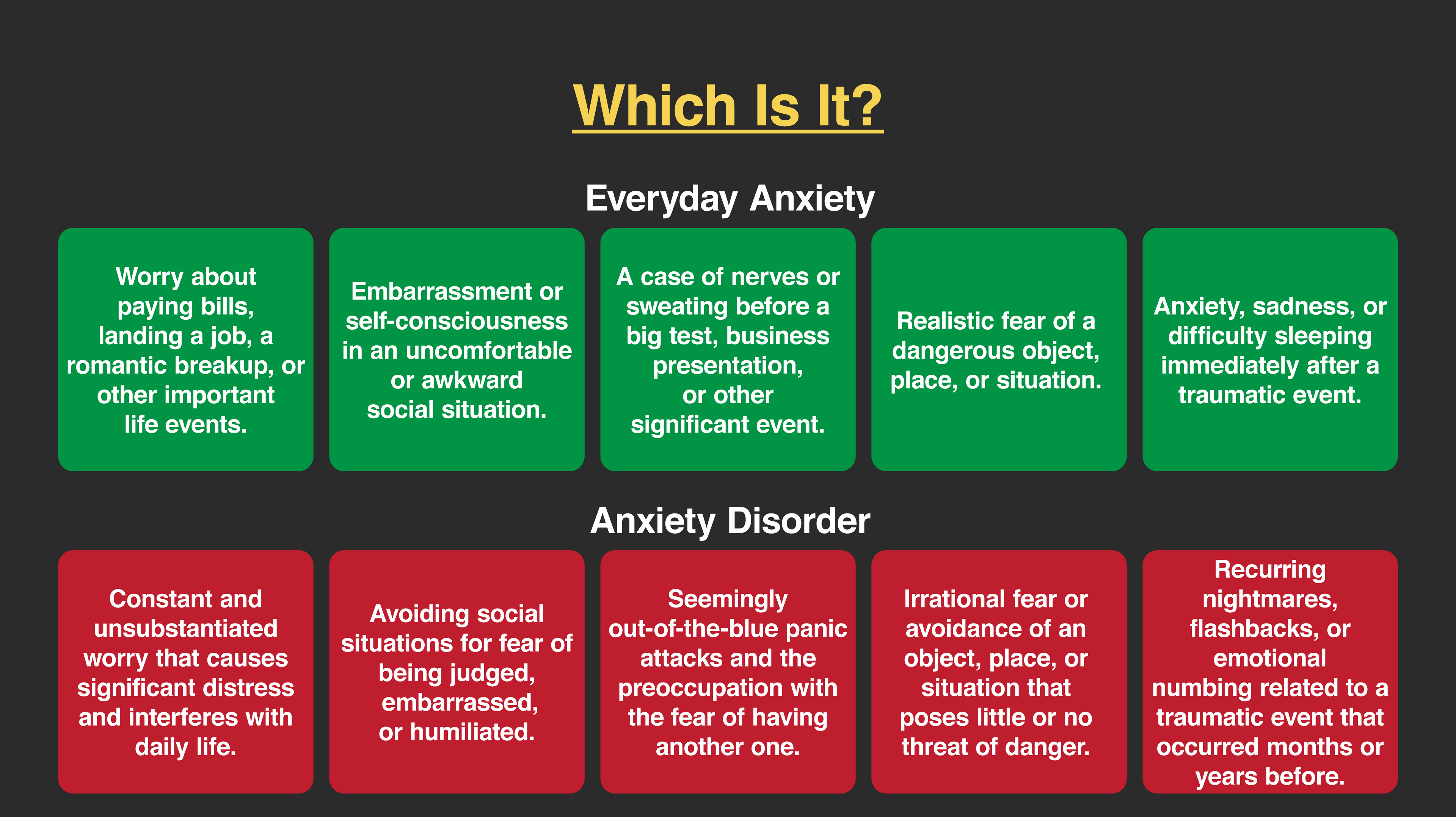
Anxiety can be a profound experience. Feelings of anxiety can range from mild apprehension to being overwhelmed and incapacitated with fear. When thinking about a heightened state of arousal in response to specific situations, it is important to distinguish between fear and anxiety. Clinically, fear is understood as a response to a danger or a real threat presented in the physical world. Anxiety, on the other hand, is the anticipation of danger but there is no actual threat present. This distinction is important because we do not want to overpathologize a completely reasonable response to something that could and even should cause a fear response. For example, if a person were robbed at a local grocery store, that experience would cause fear for most everyone. However, if that person then felt extremely anxious when they went into or even near that store later, and found themselves avoiding that store altogether, even though that store was not typically at risk for robberies, then that would be called anxiety.
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) provides our current definitions of anxiety disorders. Diagnostically speaking, for anxiety to be considered part of a disorder it must cause significant distress or impairment in social role functioning. In addition, the experience of anxiety must also be considered out of proportion to the perceived threat. That is, the anxious response must be larger than we would expect for that situation. In our example from the last chapter, if you were allergic to bees and were stung your anxious response would be very large, but that would be in proportion to the perceived threat. If, on the other hand, you were not allergic to bees and ran screaming from the room when you saw one, that response would be considered out of proportion to the perceived threat. These specifications hold true for anxiety disorders.
Phobias
Phobias are defined as an anxious response to a specific situation, object, or event. This is like our fear of bees in the example above. In the case where there is no real life-threatening outcome of being stung (although most of us can agree, it really does hurt!), that fear is really an anxiety. If the anxiety caused impairment in social role functioning or emotional distress about the possibility of being stung and it impacted one’s life negatively, then we could consider this a phobia.
There are many common types of phobias. These can range from anxiety in situations like enclosed spaces (claustrophobia), heights (acrophobia), being on planes, and even driving over bridges. There are many animal and insect phobias like a fear of dogs, birds, snakes, spiders, and of course bees. Another common type of phobia includes anxiety around needles, injections, and the sight of blood. Phobias are common in children and many phobias naturally just go away for kids. Most children who are afraid of the dark often just grow out of that. Treatments for anxiety disorders in general, and phobias specifically, are described later in this chapter.

Panic Disorder
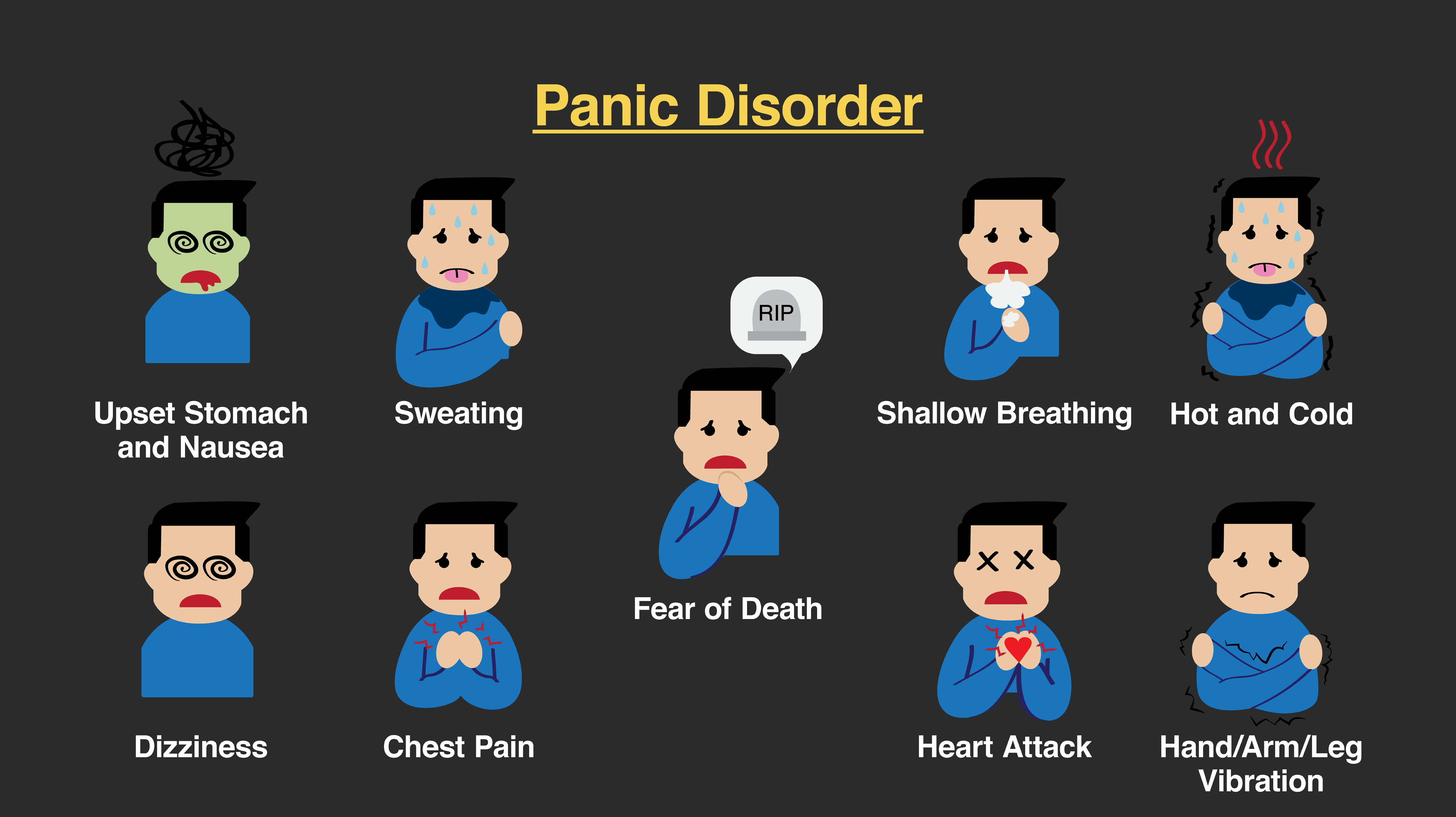
Some people have the experience of periods of overwhelming terror, where their heart is racing, they feel a shortness of breath and numbness or tingling sensations and feel out of control. These intense feelings, when not caused by a physical illness like a heart attack, are part of a panic attack. Panic attacks are discrete episodes of extreme anxiety with symptoms that last typically between 2 and 10 minutes. Panic attacks feel like they are coming out of nowhere to the person and are hard for that person to anticipate when they might happen in the future. This unpredictability adds to the anxiety of panic attacks and the associated psychological condition, panic disorder.
In order to be diagnosed with panic disorder, the person needs to have at least one panic attack and often is then afraid of having more attacks in the future. Panic disorder is experienced with great distress by those who struggle with it. While some people experience one panic attack and do not go on to develop the disorder, many do go on to have more panic attacks and the anxiety of recurrent attacks. This anticipation of additional attacks can cause a gradual closing in of places the person will go. In fact, some people with panic disorder struggle with leaving the house, a condition known as agoraphobia.
It is important to recognize that these attacks are not caused or made worse by a physical disorder. For example, if a person has an overactive thyroid gland (called hyperthyroidism), he or she may experience panic-like symptoms. In this situation, however, the person would not be diagnosed with panic disorder, and a physician would treat the thyroid problem. This is also the case for some heart conditions that can create panic-like symptoms. Some drugs (both legal and illegal) can cause a person to feel panic symptoms including high doses of caffeine, stimulants like prescribed amphetamine for psychological conditions, as well as illegal drugs like cocaine and methamphetamine. It is essential that mental health professionals rule out physical causes of what may appear to be panic attacks and treat those problems or diseases appropriately.
Obsessive-compulsive Disorders
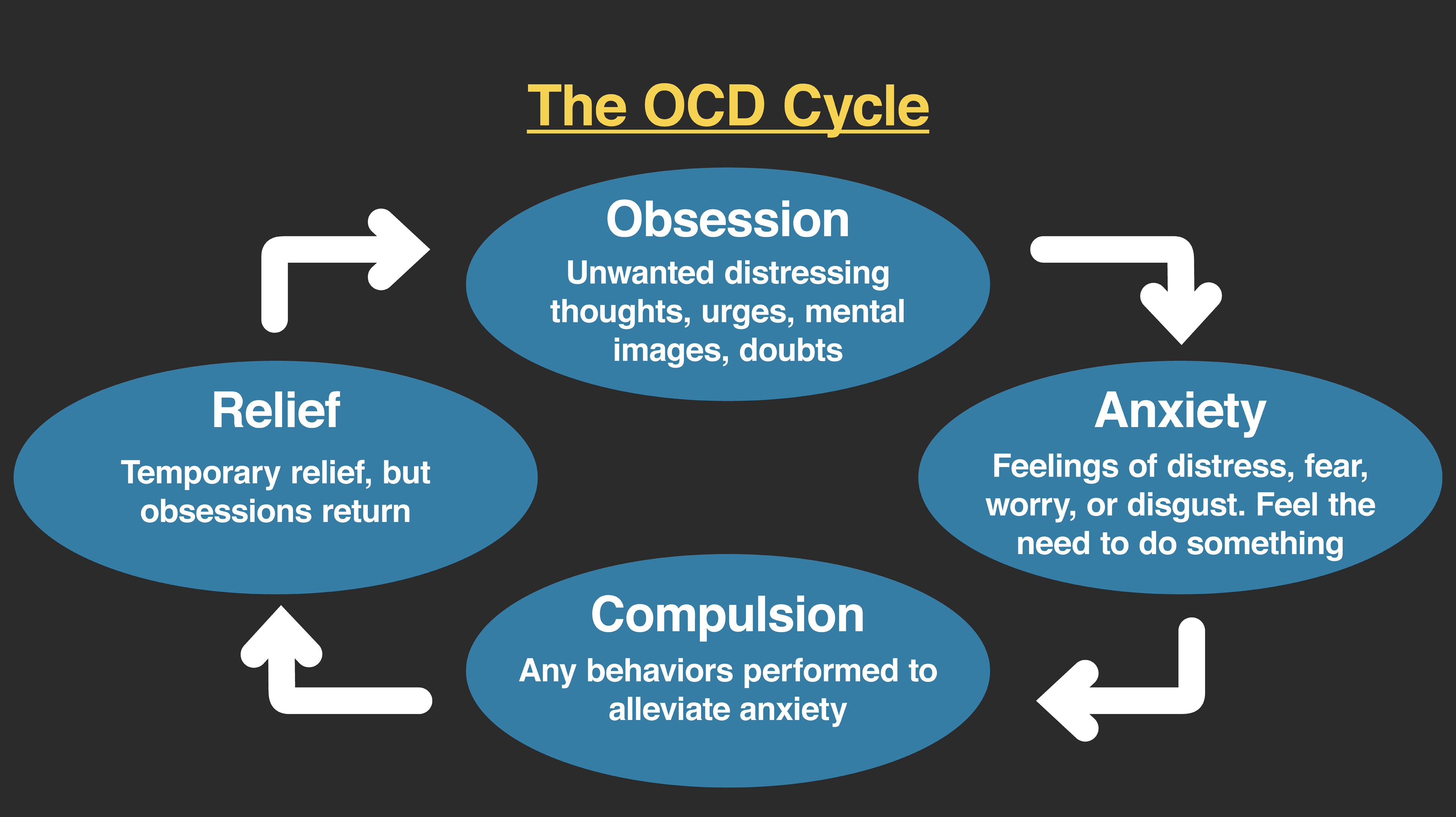
The DSM-5 considers obsessive-compulsive disorder (OCD) to be in its own category with a few other disorders (e.g., hoarding, body dysmorphic disorder), but until the recent edition of the DSM, it was categorized as an anxiety disorder. Most people understand OCD as an anxiety problem. OCD is characterized by obsessions and compulsions. Diagnostically, obsessions are thoughts, images, or ideas that the person experiences as unwanted and intrusive. That is, an obsession is not just something we are excited about or interested in, it is the experience of a thought or impulse or image that feels like it cannot be stopped. Importantly, the person recognizes that the thought is his or her own but feels like it occurs out of his or her control. Common obsessions include fears of being contaminated, of harming others or being harmed, and inappropriate sexual content.
Compulsions are acts performed in response to obsessions. These are often rituals that are designed to reduce the anxiety associated with the obsessive image or idea. Common compulsions can include washing or bathing rituals, checking, counting, and other behaviors designed to prevent harm from coming to a person. While compulsions are often tied to obsessions, there is sometimes a more magical or unrealistic aspect to the act in its relation to the intrusive thoughts. For example, if a person has a checking compulsion in response to a fear that the coffee pot could cause a fire if left plugged in (which would be very uncommon in most modern houses), the checking ritual would likely be quite elaborate and might involve unplugging and plugging back in the cord numerous times. Compulsions can be very time-consuming for those struggling with OCD and can be embarrassing to the individual.
While it is not required that both obsessions and compulsions be present, it is common to see them together. Most individuals who seek treatment have thoughts or images that are hard for them to get rid of, and they engage in some ritual to try to provide temporary relief from their distress. Interestingly, even though a ritual like counting or checking or washing hands can take an edge off of the person’s anxiety temporarily, the compulsive action does not prevent the obsessive thought from occurring again. In fact, oftentimes the compulsive act has to be done to an even larger degree over time (e.g., washing for longer or with hotter water) in response to obsessive thoughts.
Posttraumatic Stress Disorder
Posttraumatic stress disorder (PTSD) is now categorized into its own section of the DSM-5 called Trauma- and Stressor-Related Disorders. PTSD is characterized by a complex number of symptoms that follow either experiencing or witnessing an event that is overwhelming and where the person’s safety may have been gravely endangered. Following this experience, the person then feels like the experience is happening again (through flashbacks or nightmares) and has intrusive thoughts about the event. PTSD also involves an increased arousal level where the person feels like they are on edge or keyed up, almost as if being prepared for imminent danger. There are also changes in the types of thoughts and feelings that the person has following the trauma including a loss of interest in activities and a sense of disconnection or estrangement from others. Finally, the person also engages in physical or emotional avoidance of stimuli that are associated with the traumatic event. All of these groups of symptoms must be met to be diagnosed with PTSD, and they must occur for at least one month. When these behaviors occur for less than one month, they are called acute stress disorders.
PTSD has been studied under one label or another (e.g., shell shock, battle fatigue, Gulf War Syndrome) for many years. In the last several decades, however, the research on what we now call PTSD has yielded very useful information. For example, we know that on average both men and women experience traumatic events. While men experience more of these events, women are more often diagnosed with PTSD, in part because women are more likely to disclose difficulties with their psychological experiences. We know that rates for being diagnosed with PTSD are higher for some types of traumatic experiences than others (e.g., combat exposure, natural disasters, sexual assault, childhood sexual abuse). We also know that individuals diagnosed with PTSD are likely to abuse drugs or alcohol in an attempt to try to cope with their distress, and we know that there can be high suicide rates with some populations who have experienced trauma (e.g. military veterans).

Treatment of Anxiety Disorders
- Cognitive Behavior Therapy (CBT)
- Associative learning
- Dog phobia
- Flight as an ineffective remedy
- Exposure
- Exposure therapy techniques
- Relaxation
- Exposure with Response Prevention (EBT)
Section Focus Question:
How is CBT used to cure anxiety disorders?
Key Terms:
The treatment of anxiety disorders has been at the forefront of psychopathology for over one hundred years. People like Sigmund Freud hypothesized that anxiety from the unconscious mind was to be understood through years of psychoanalytic interpretation to get to the true underlying cause of the person’s problems. Today, most of the scientific data indicates that the most effective treatments for anxiety disorders are from a cognitive and behavioral framework. Cognitive behavior therapy (CBT) as outlined in the previous chapter is an approach to understand and treat psychological problems using a combination of both cognitive therapy approaches and behavioral intervention strategies.
Behavior Therapy
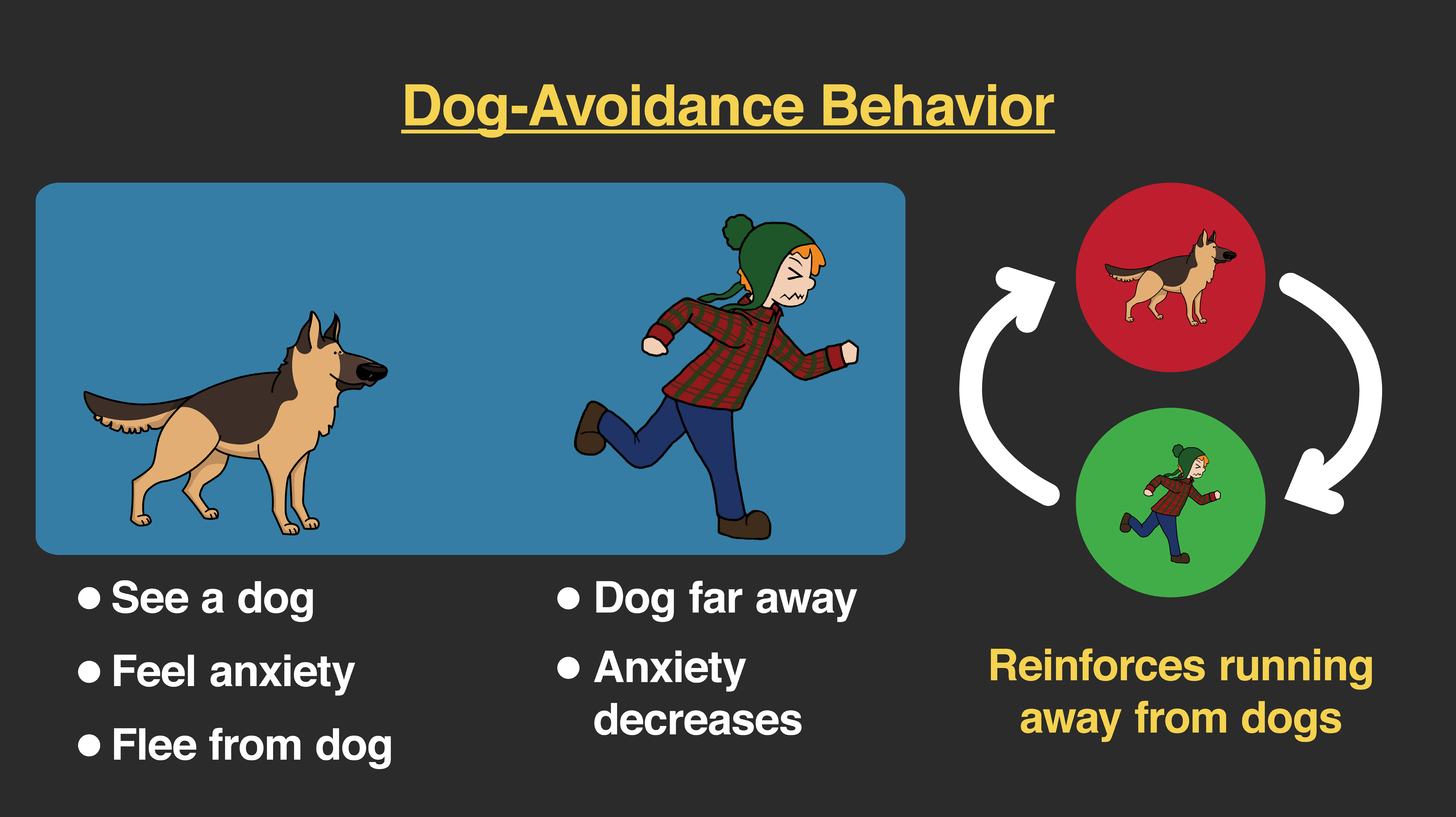
From a behavioral standpoint, anxiety is a natural response to having experienced some aversive or distressing event. In other words, we have learned through classical conditioning (associative learning) that some stimuli are associated with aversive (painful, scary, and so on) experiences. These conditioned stimuli give rise to emotions that are similar to the original events that understandably caused that pain or fear. This associative learning can be used to understand a great deal of the anxiety disorders we have discussed. For example, a dog phobia (a conditioned response to the conditioned stimulus of a dog) would be a natural outcome to having been bitten by or even caused to be very afraid of a dog in the past (unconditioned stimulus of being bitten and unconditioned response of fear and pain). This would also be true of stimuli associated with a traumatic event such as in a car accident (an unconditioned stimulus giving rise to fear), where a person may feel anxiety (a conditioned response) when getting back into the car (conditioned stimulus).
These associated cues that cause a person to feel very anxious when the actual threatening event is no longer present are also wrapped up in instrumental (or operant) learning responses. When we see the dog and feel anxious, we escape that situation, and that escape behavior is negatively reinforced; by removing an aversive experience, we are more likely to escape in similar situations. More than that, we will try to avoid dogs at all costs. This, too, is negatively reinforced behavior, as any anxiety surrounding the anticipation of encountering a dog is reduced by the decision not to be near one in the future. Again, the same behavioral principles are used to understand the avoidant behaviors we see in PTSD with stimuli associated with the traumatic event. This is also true for the compulsive rituals we find in OCD. A ritual is repeatedly done in an effort to reduce the anxiety that comes with an obsession. Even though the compulsive activity may be arbitrarily tied to the obsession, the person performs that compulsive act to escape the aversive feelings associated with those thoughts.
There are many problems associated with negatively reinforced escape and avoidance behaviors. When we do something to get rid of thought or feeling, it can only work for a short amount of time. That thought or emotion will return, and when it does, it sometimes comes back even stronger. This requires, even more, escape behavior which can look like more withdrawal, more avoidance, or in the case of OCD, even more, intense compulsive rituals. More than this, the person can often end up feeling disconnected from others, living a life that is not in line with his or her values, or without much real pleasure in living.
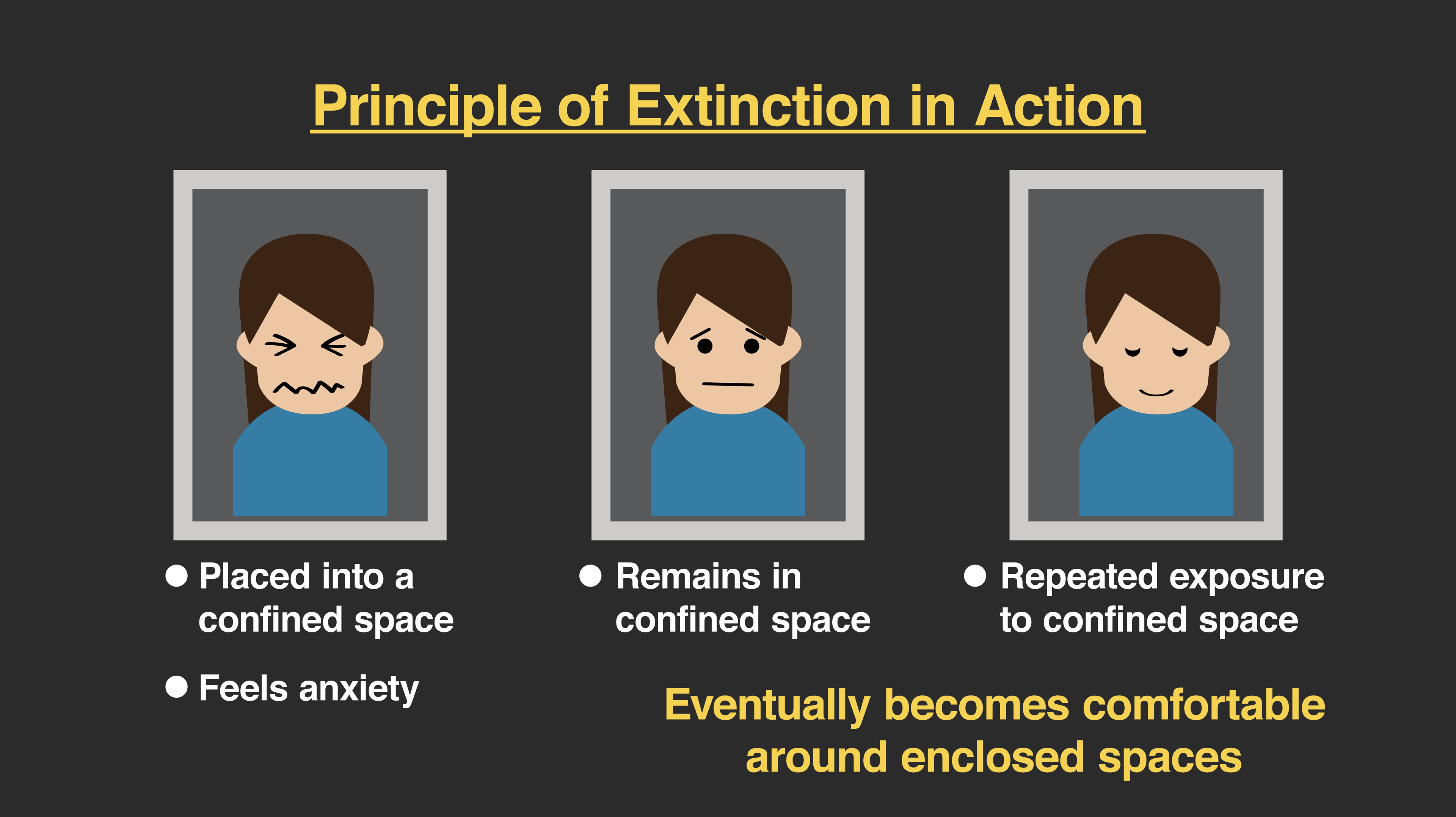
The treatments for anxiety disorders now center dominantly on the concept of exposure. In order to break the back of anxiety, the person needs to be exposed to that which seems most scary. While this sounds intense and even frightening, the reality is that there are now many studies showing that anxiety responses are dramatically reduced by the principles of extinction. Using classical conditioning models, if we present the conditioned stimuli (the things that cause anxiety) without the unconditioned stimuli, that association between the two is weakened. In other words, seeing a dog that would normally scare us no longer produces anxiety because it is not associated with danger. In anxiety disorder terms, if we allow a person to be anxious in a situation like a closed space (claustrophobia), but nothing bad occurs to that person, then that closed space no longer signals anxiety.
From an operant framework, we focus on the role of escape and avoidance behaviors that have been negatively reinforced and prevent those from continuing. The goal here is to expose the person to the feared stimuli that would cause the client to escape and ask him or her to experience the anxiety. With repeated practice, the anxious feelings that would normally make the person want to get away from the situation become not only tolerable, but those feelings decrease in intensity and eventually go away. An important part of exposure therapy is to help the client learn relaxation skills so that the body is less likely to be triggered into a fight or flight response that comes with escaping. These relaxation skills create a physiological state that is incompatible with anxiety and allows the client to engage in more effective behaviors when he or she is anxious and feels the need to escape. Exposure therapy is the cornerstone to most contemporary interventions for anxiety disorders.
Let’s consider a few examples that use exposure therapy. In OCD, the most effective treatment is called exposure with response prevention (ERP). ERP, as you can guess from its name, centers on exposing the client to feared stimuli and then prevents the person from engaging in an escape response. If a client is afraid of contamination and engages in a handwashing ritual to try to soothe their obsession, then the mental health professional’s job is to trigger those obsessions (and the need to perform their compulsive acts) by having the client engage those stimuli. Specifically, if that client were afraid to touch a kitchen counter because it might be contaminated, then the client would be required to go ahead and touch that counter, to interact with and use it the way anyone would normally but not engage in the compulsive response designed to reduce that anxiety. With practice, the escape response is extinguished and along with it, the anxiety in response to the associated stimuli.
This type of exposure occurs similarly with phobias as it does for panic disorder and for PTSD. Notice that with PTSD there are both physical triggers (e.g., anxiety in response to being around a man after a sexual assault or loud noises after a combat injury) and psychological triggers. A client with PTSD can be triggered by memories or images related to the trauma, and the exposure work centers on those stimuli. In this case, the client may escape or avoid by becoming more disconnected from his or her feelings or by using drugs or other substances to temporarily stop those experiences. Mental health professionals working with clients with trauma will have the client engage their feared memories, thoughts, and emotions and not escape. Coupled with relaxation skills, exposure can allow the memories to become experienced as memories, rather than stimuli that cannot be tolerated and must be avoided or escaped.
Cognitive Therapy
- Cognitive therapy for panic attacks
- Combination of cognitive and exposure therapies
- Sympathetic nervous system
- Relaxation breathing
- Neck stretching
- Various exercises for relaxation
- Cognitive Behavior Therapy (CBT)
Section Focus Question:
What is the nature of a panic attack and what can be done about it?
Key Terms:
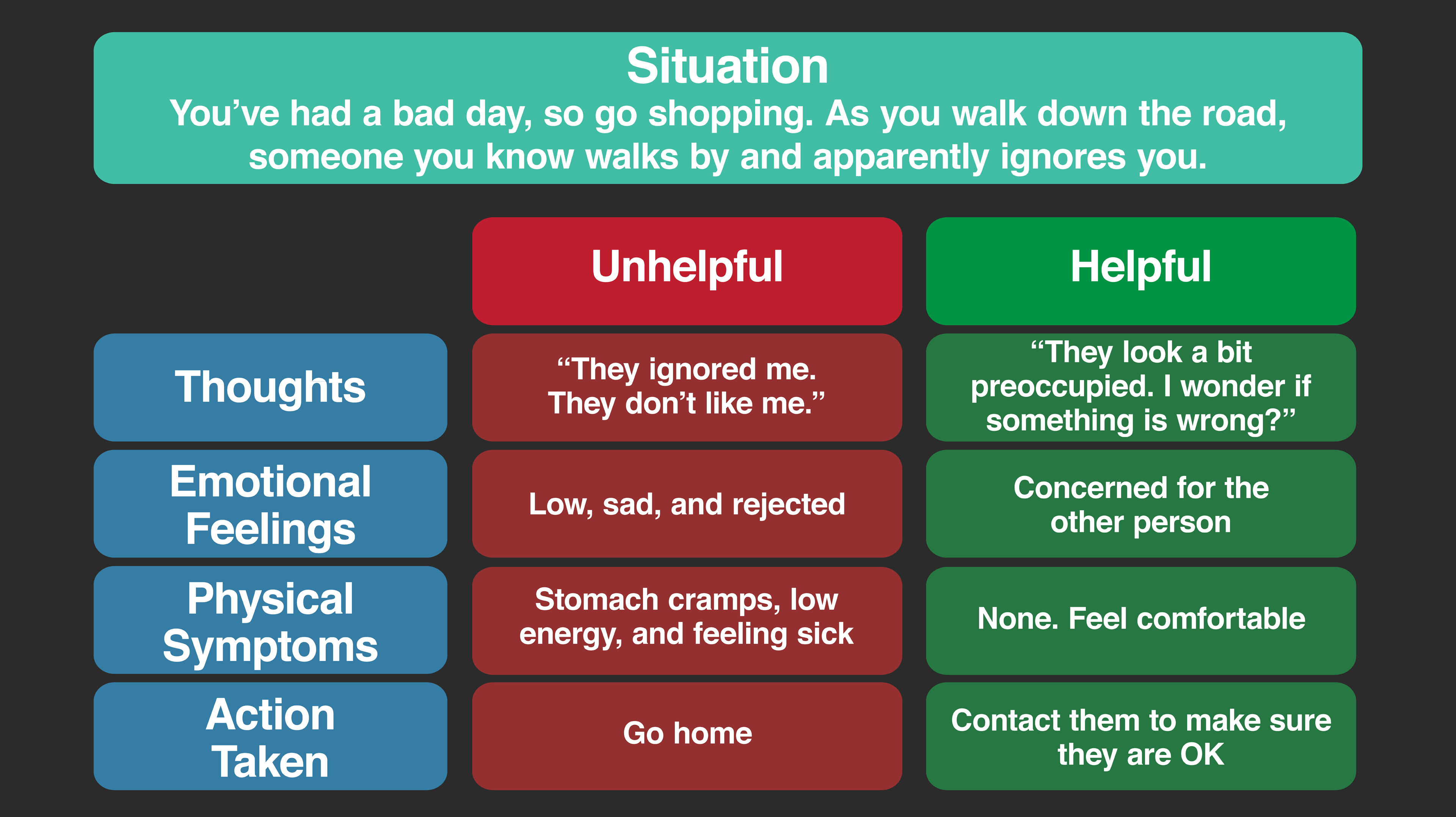
Frequently, cognitive therapy is combined with behavior therapy as part of traditional CBT interventions. Cognitive therapy approaches focus on the core schemas related to feared situations, memories, or experiences. These core schemas result from the difficult situations that a person encounters and give rise to problematic behaviors and difficult emotional experiences. As discussed in the previous chapter, cognitive therapy seeks to challenge negative automatic thoughts and replace dysfunctional core schema with more accurate beliefs. By replacing these dysfunctional schemas with more accurate thinking patterns, the client will ultimately feel better and behave more effectively.
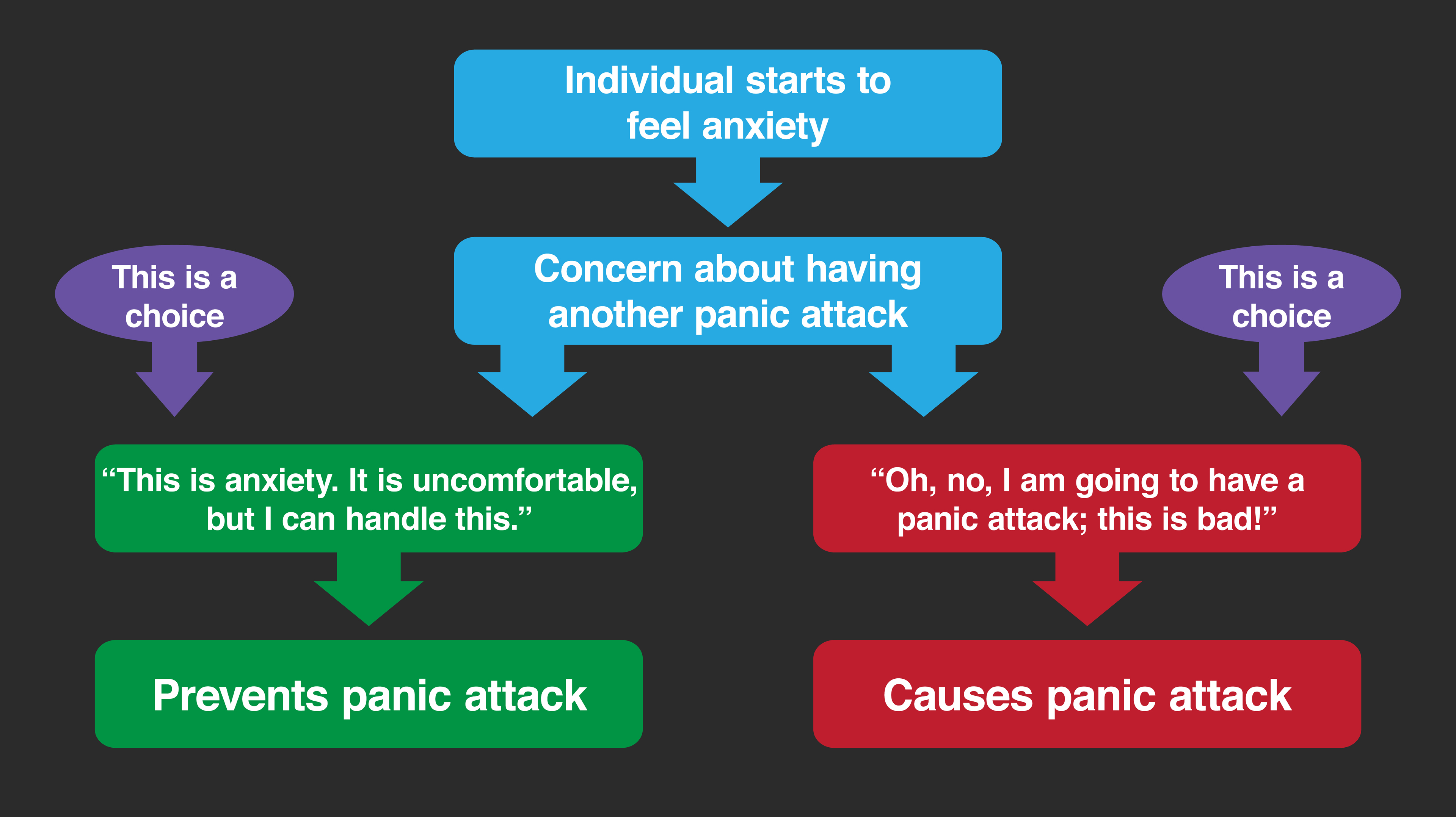
Consider, as an example, a cognitive model of panic disorder. People who have had panic attacks often live in fear of having another attack. They will begin to feel some anxiety and then tell themselves that a panic attack is going to happen, that they cannot stop it, and they will be incapacitated when it occurs. In fact, when a person feels anxious and has the thought, “Oh, no, I am going to have a panic attack; this is bad,” that will actually help increase his or her physiological arousal enough so that the full panic attack happens.
A cognitive therapist will help the client learn about panic attacks from a psychological as well as physiological perspective, and then help him or her challenge those thoughts when they occur, replacing them with more accurate beliefs. This is most often coupled with exposure therapy. During the exposure process, when the client’s emotions are triggered with gradually increasing amounts of anxiety, the client is encouraged to practice thinking something like, “This is anxiety. It is uncomfortable, but I can handle this. My hands are sweating and my heart is racing, but that is a natural response to feeling this arousal. It does not mean that I will panic. But if I do, I can handle this.” The client is encouraged to practice relaxation skills, including deep breathing so that he or she is less likely to engage in a panic attack and continues with the exposure to cues the therapist identifies as triggering panic for that person.
The cognitive model for the other anxiety disorders is similar to that with panic and centers on changing dysfunctional core beliefs. In the case of PTSD, many CBT approaches focus on the importance of challenging newly developed dysfunctional fear schemas. These are understandable reactions, but often are very inaccurate schema and limit the person in where they are willing to go, who they can be around, and ultimately cause a great deal of suffering. For example, if a person were sexually assaulted, it would make sense if that client developed a core belief like, “the world is dangerous,” or “men (or women) are out to harm me.” Even though we can imagine where these thoughts come from, and they may temporarily help the person stay out of risky situations, ultimately they are not accurate, and they may prevent the person from engaging in life the way he or she used to be able to do.
The therapist doing CBT for PTSD will focus on helping challenge and replace those dysfunctional beliefs with more accurate ones. This would be done in the context of both exposure-based treatments to the feared thoughts or memories and learning strategies to better ensure the safety of the client. Prolonged exposure and cognitive processing therapy are both contemporary examples of CBT treatments that have excellent data for their efficacy and are on the forefront of effective interventions for trauma- and stressor-related disorders.